About pLGG
Favorable prognosis, real risk for recurrence/
Easton, lives with pLGG.
Lives for painting.
Pediatric low-grade glioma (pLGG) is the most common type of brain tumor in children2
With an incidence rate of 3.83 per 100,000, the most frequently diagnosed solid malignant tumors in children occur in the brain and CNS3
pLGG accounts for about 30% of all childhood CNS tumors, with pilocytic astrocytoma constituting the majority of cases2,4,5
Pilocytic astrocytoma occurs mainly in children and young adults aged 5 to 19 years, with a peak incidence in the 5- to 9-year-old range6
pLGG has a 10-year OS over 90%. However, the disease progresses in about 50% of diagnosed children after initial treatment and requires adjuvant therapy.2
Localized symptoms are typically characteristic of tumor location.6*



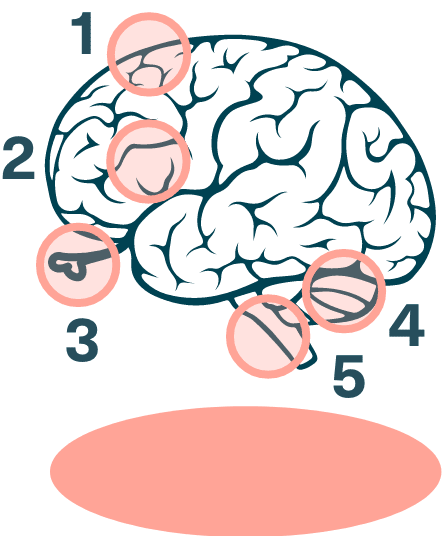
1
Cerebral gliomas:
seizures, hemiparesis (weakness on one side of the body), and behavioral changes
2
Hypothalamus gliomas:
endocrine dysfunction and visual deficits
3
Optic pathway gliomas:
decreased visual acuity, proptosis (bulging of the eyes), and strabismus (misalignment of the eyes)
4
Cerebellar gliomas:
ataxia (impaired balance or coordination) and dysmetria (impaired perception of depth and distance)
5
Brain stem gliomas:
dysphasia (difficulty swallowing), dysarthria (weakness of muscles used for speech), and abnormal breathing
*Not a comprehensive list.
Despite favorable prognosis, relapse or progression occurs in about half of patients with pLGG and may require multiple rounds of therapy.2
CNS=central nervous system; OS=overall survival.
Back to TopReferences: 1. Ryall S, Zapotocky M, Fukuoka K, et al. Integrated molecular and clinical analysis of 1,000 pediatric low-grade gliomas. Cancer Cell. 2020;37(4):569-583.e5. doi:10.1016/j.ccell.2020.03.011 2. Ryall S, Tabori U, Hawkins C. Pediatric low-grade glioma in the era of molecular diagnostics. Acta Neuropathol Commun. 2020;8(1):30. doi:10.1186/s40478-020-00902-z 3. Ostrom QT, Cioffi G, Gittleman H, et al. CBTRUS Statistical Report: primary brain and other central nervous system tumors diagnosed in the United States in 2012-2016. Neuro Oncol. 2019;21(Suppl 5):v1-v100. doi:10.1093/neuonc/noz150 4. Ostrom QT, Patil N, Cioffi G, Waite K, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report: Primary brain and other central nervous system tumors diagnosed in the United States in 2013-2017 [published correction appears in Neuro Oncol. 2022;24(7):1214]. Neuro Oncol. 2020;22(12 suppl 2):iv1-iv96. doi:10.1093/neuonc/noaa200 5. Bandopadhayay P, Bergthold G, London WB, et al. Long-term outcome of 4,040 children diagnosed with pediatric low-grade gliomas: an analysis of the Surveillance Epidemiology and End Results (SEER) database. Pediatr Blood Cancer. 2014;61(7):1173-1179. doi:10.1002/pbc.24958 6. Sievert AJ, Fisher MJ. Pediatric low-grade gliomas. J Child Neurol. 2009;24(11):1397-1408. doi:10.1177/0883073809342005 7. Collins KL, Pollack IF. Pediatric low-grade gliomas. Cancers (Basel). 2020;12(5):1152. doi:10.3390/cancers12051152