BRAF Alterations
BRAF alterations (fusion or mutation)
in the MAPK pathway
Lily, lives with pLGG.
Lives for dancing.
The MAPK pathway is a key regulator of cell proliferation, survival, and differentiation6
In normal cells, the pathway is tightly regulated. BRAF is activated by RAS and relays signals via MEK and ERK7
However, when BRAF is altered, the pathway is unregulated, leading to increased, continuous signaling, independent of RAS. This can occur from a BRAF gene fusion or point mutation6-8
Explore BRAF in the MAPK pathway for pediatric low-grade glioma (pLGG)
Activating BRAF alterations are the most common oncogenic driver of pLGG3
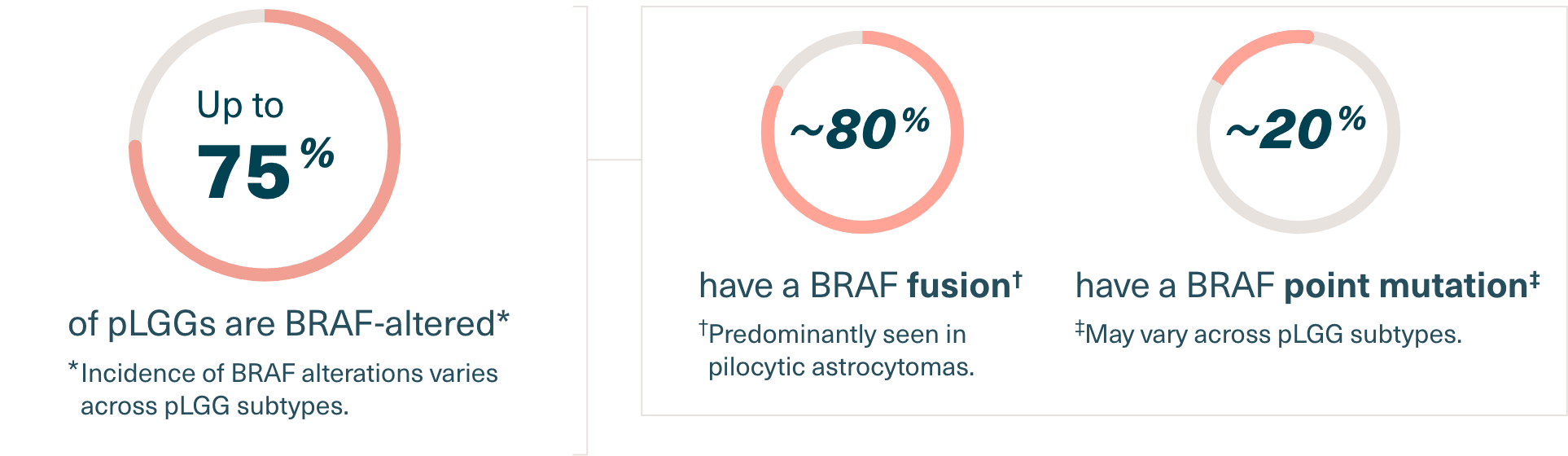
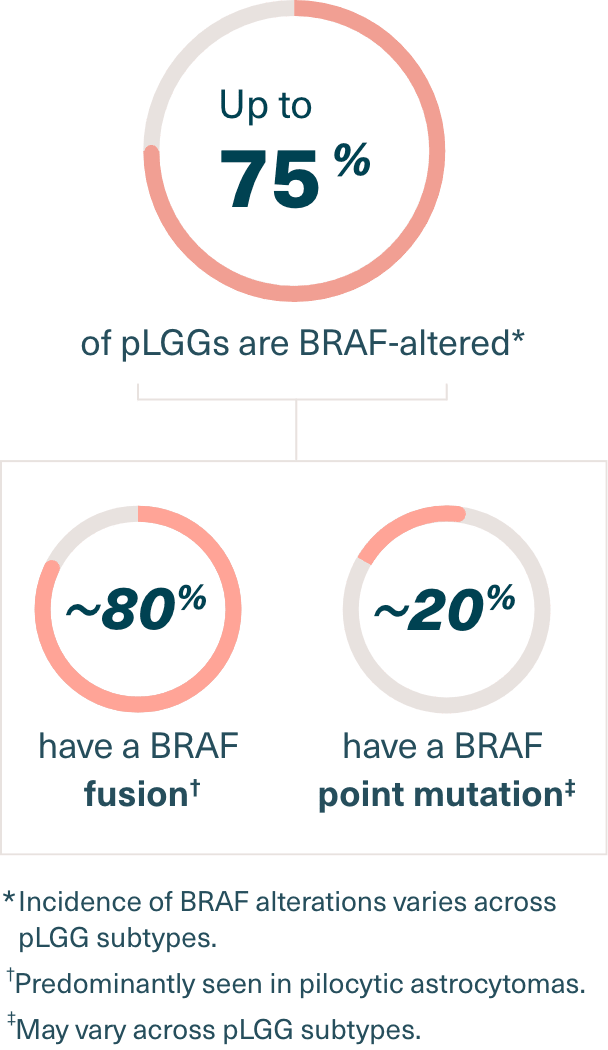
Up to 75% of pLGG have a BRAF alteration (fusion or mutation). Of these, approximately 80% have a BRAF fusion, while approximately 20% have a BRAF point mutation.9-13
BRAF-altered pLGG9-13


Knowing if your patient’s pLGG harbors a BRAF fusion or point mutation is critical as it may help determine an appropriate targeted therapy.4
References: 1. Hauser P. Classification and treatment of pediatric gliomas in the molecular era. Children (Basel). 2021;8(9):739. doi:10.3390/children8090739 2. Louis DN, Perry A, Wesseling P, et al. The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol. 2021;23(8):1231-1251. doi:10.1093/neuonc/noab106 3. Ryall S, Tabori U, Hawkins C. Pediatric low-grade glioma in the era of molecular diagnostics. Acta Neuropathol Commun. 2020;8(1):30. doi:100.1186/s40478-020-00902-z 4. Behling F, Schittenhelm J. Oncogenic BRAF alterations and their role in brain tumors. Cancers (Basel). 2019;11(6):794. doi:10.3390/cancers11060794 5. Andrews LJ, Thornton ZA, Saincher SS. Prevalence of BRAF V600E in glioma and use of BRAF inhibitors in patients with BRAF V600E mutation-positive glioma: systemic review. Neuro Oncol. 2022; 24(4):528-540. doi:10.1093/neuonc/noab247 6. Sholl LM. A narrative review of BRAF alterations in human tumors: diagnostic and predictive implications. Precis Cancer Med. 2020; 3(26);1-15. doi: 10.21037/pcm-20-39 7. Yaeger R, Corcoran RB. Targeting alterations in the RAF-MEK pathway. Cancer Discov. 2019;9(3):329-341. doi:10.1158/2159-8290.CD-18-1321 8. Srinivasa K, Cross KA, Dahiya S. BRAF alterations in central and peripheral nervous system tumors. Front Oncol. 2020;10:574974. doi:10.3389/fonc.2020.574974 9. Sun Y, Alberta JA, Pilarz C. A brain-penetrant RAF dimer antagonist for the noncanonical BRAF oncoprotein of pediatric low-grade astrocytomas. Neuro Oncol. 2017;19(6):774-785. doi:10.1093/neuonc/now261 10. Penman CL, Faulkner C, Lowis SP, Kurian KM. Current understanding of BRAF alterations in diagnosis, prognosis, and therapeutic targeting in pediatric low-grade gliomas. Front Oncol. 2015;5:54. doi:10.3389/fonc.2015.00054 11. Ryall S, Zapotocky M, Fukuoka K, et al. Integrated molecular and clinical analysis of 1,000 pediatric low-grade gliomas. Cancer Cell. 2020;37(4):569-583.e5. doi:10.1016/j.ccell.2020.03.011 12. Cohen AR. Brain tumors in children. N Engl J Med. 2020; 386(20):1922-1931. doi:10.1056/NEJMra2116344 13. Lassaletta A, Zapotocky M, Mistry M, et al. Therapeutic and prognostic implications of BRAF V600E in pediatric low-grade gliomas. J Clin Oncol. 2017;35(25):2934-2941. doi:10.1200/JCO.2016.71.8726